INTRODUCTION
The room is pitch black, save for the cool, blue glow of high-resolution monitors. A radiologist sits in the silence, staring at a mammogram. To the untrained eye, the image is just a chaotic smudge of grey, white, and black clouds. But to the radiologist, it is a map of a human life.
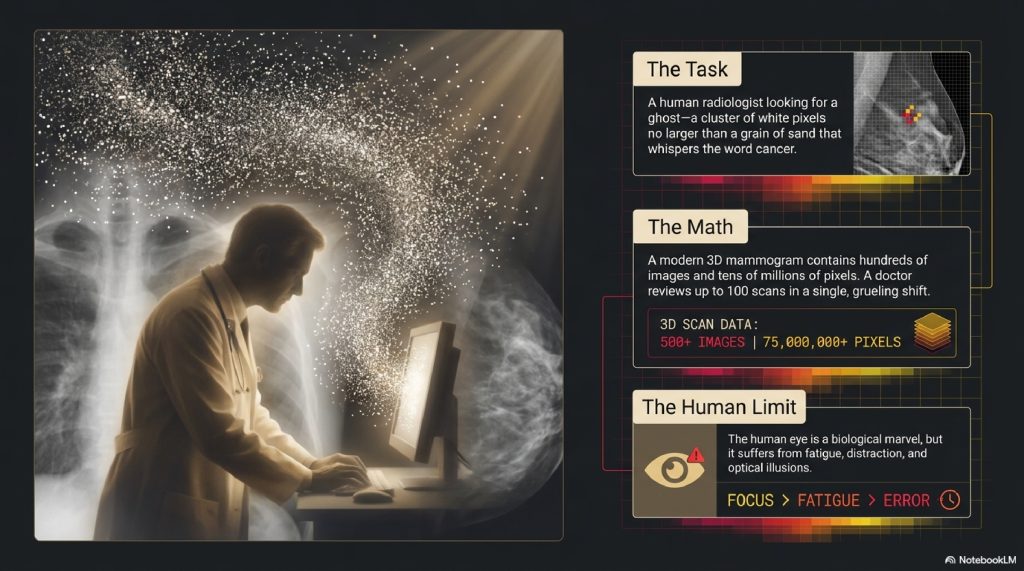
They are looking for a ghost. They are searching for a cluster of white pixels perhaps no larger than a grain of sand that shouldn’t be there. A tiny architectural distortion in the breast tissue that whispers the word cancer.
Now, consider the math: A modern 3D mammogram contains hundreds of individual images, totaling tens of millions of pixels. A radiologist might review a hundred of these scans in a single, grueling shift. The human eye is a biological marvel, but it gets tired. It suffers from fatigue, distraction, and optical illusions.
What if there was a second set of eyes? A set of eyes that never sleeps, never needs a coffee break, and has memorized the exact microscopic pixel patterns of one million previous cancer cases?
Welcome to the medical revolution of Artificial Intelligence.
We often hear that AI is “reading X-rays” or “diagnosing patients,” but the mainstream media rarely explains how. It’s treated like magic. A scan goes into a black box, the computer blinks, and a diagnosis pops out. But there is no magic. There is only a masterclass in geometry, pattern recognition, and billions of mathematical calculations happening in the blink of an eye.
Today, we are going to strip away the hype and open up the black box. We will travel down to the level of the individual pixel to see exactly how a machine learns to “see” illness. We will explore the neural networks that mimic the human brain, and reveal why the future of medicine isn’t about computers replacing doctors, it’s about giving doctors a digital superpower.
Take a deep breath. Let’s look inside.
TABLE OF CONTENTS
- The Simple Explanation: The World’s Fastest Art Critic
- Step-by-Step: The Journey of a Medical Scan
- Real-World Example: Catching the Invisible Lung Tumor
- The Advanced Technical Layer: How CNNs Actually Work
- Common Myths About AI in Medicine
- The Future: Predicting the Unpredictable
- Fascinating Facts You Didn’t Know
- FAQs
- Other Blog Suggestions
- Conclusion
A. THE SIMPLE EXPLANATION: The World’s Fastest Art Critic
To understand how AI reads a medical scan, imagine an art critic whose entire job is to spot forged paintings.
If you or I look at a forged painting, we look at the whole picture. We see a portrait of a person, and it looks pretty good to us.
But the elite art critic doesn’t look at the person. They pull out a magnifying glass and look at the brushstrokes. They know that the original artist always flicked their wrist at a 45-degree angle when painting shadows. The forger flicked their wrist at a 40-degree angle. The difference is invisible from a distance, but glaring under a microscope.
An AI is that elite art critic.
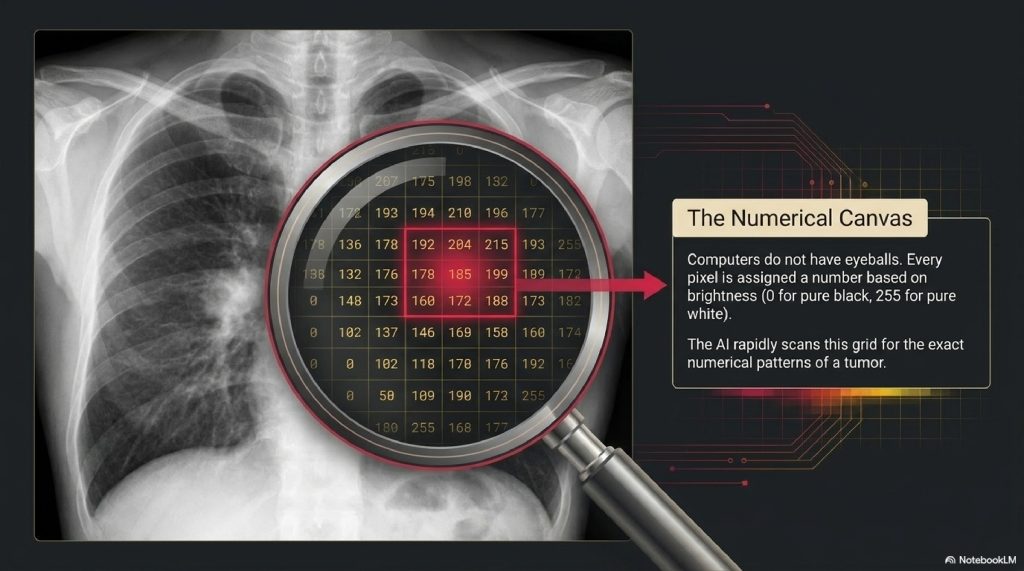
When an AI looks at an MRI or an X-ray, it doesn’t see a “lung” or a “brain.” Computers don’t have eyeballs or concepts of human anatomy. The AI sees a massive grid of numbers. Every single pixel in the image is assigned a number based on how bright or dark it is (usually from 0 for pure black, to 255 for pure white).
The AI has been trained on millions of previous scans where human doctors have meticulously circled tumors. By grinding through the math, the AI has learned that tumors contain a very specific sequence of numbers (brushstrokes) at their edges. When you feed it a new scan, it rapidly scans the grid, looking for that exact numerical pattern.

B. STEP-BY-STEP BREAKDOWN: The Journey of a Scan
What actually happens in the seconds after a patient slides out of an MRI machine? The AI performs a highly choreographed, four-step routine.
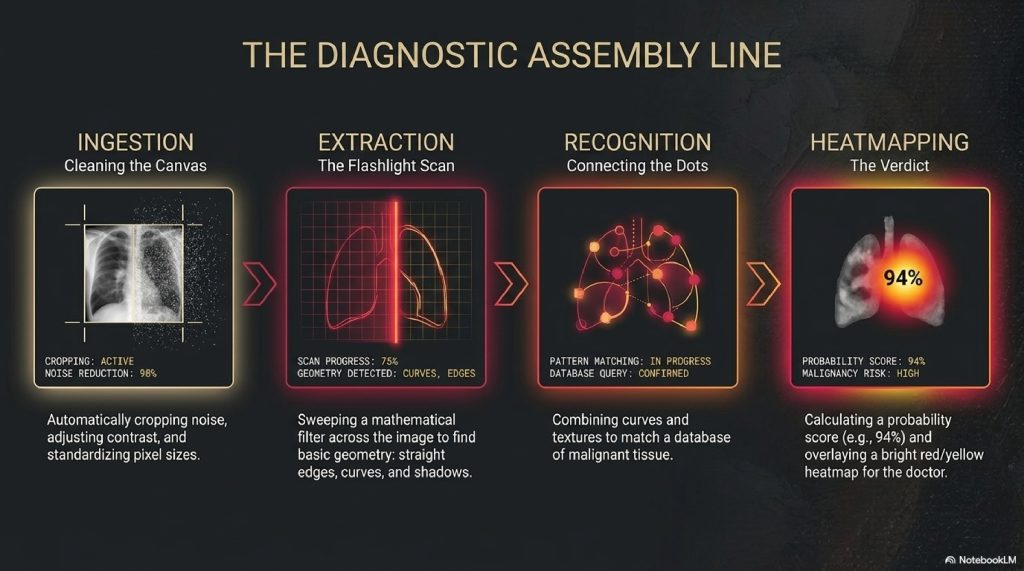
Step 1: Ingestion and Pre-Processing (Cleaning the Canvas) Medical scans come from different machines, hospitals, and lighting conditions. Before the AI can read the scan, it has to standardize it. The algorithm automatically crops out background noise, adjusts the contrast, and standardizes the pixel sizes so it has a perfectly clean, uniform canvas to analyze.
Step 2: Feature Extraction (The Flashlight Scan) This is the heavy lifting. The AI takes a digital “flashlight” (a mathematical filter) and sweeps it across the image, pixel by pixel, top to bottom. It isn’t looking for a disease yet. It is looking for basic geometric features: straight edges, curves, shadows, and textures.
Step 3: Pattern Recognition (Connecting the Dots) Once the AI has mapped all the curves and edges, deeper layers of the algorithm start combining them. It realizes that a certain curve connected to a specific shadow creates a texture that matches a database of malignant tissue.
Step 4: Classification and Heatmapping (The Verdict) The AI calculates a probability score. It says, “There is a 94% mathematical probability that the pixels in the upper right quadrant represent a lesion.” It doesn’t just print a report; it generates a “Heatmap,” overlaying bright red or yellow colors onto the original image so the human doctor knows exactly where to look.
C. REAL-WORLD EXAMPLES: Catching the Invisible Lung Tumor
Let’s look at low-dose CT scans used for lung cancer screening.
Lung cancer is notoriously deadly because by the time a patient feels symptoms, the cancer has usually spread. Catching a tiny, millimeter-sized lung nodule early can be the difference between life and death.
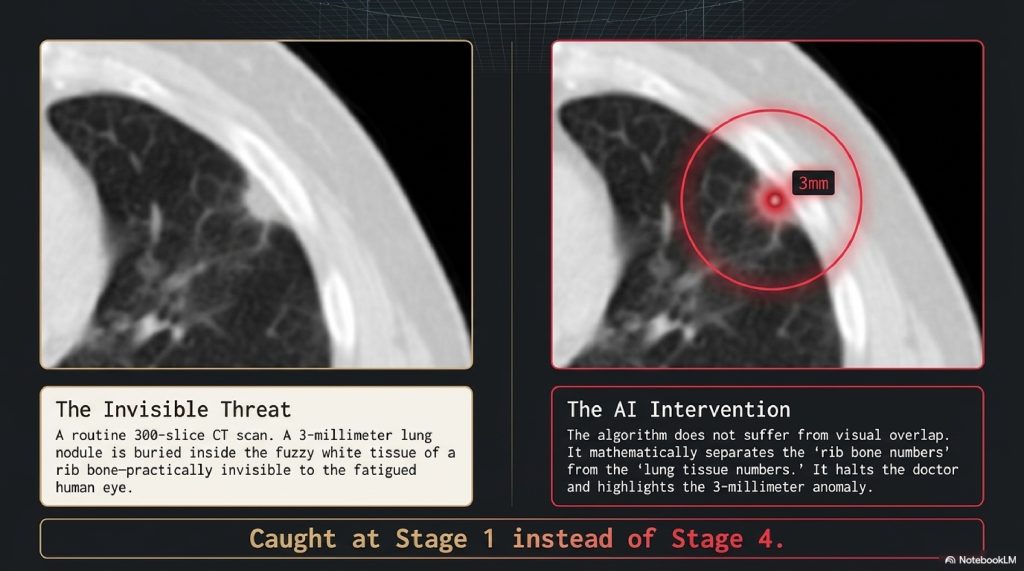
Imagine a 60-year-old patient gets a routine CT scan. The scan creates 300 different image “slices” of their lungs. A radiologist scrolls through these 300 images. Tucked behind a rib bone, buried in the fuzzy white tissue of a blood vessel, is a nodule measuring exactly 3 millimeters. It is practically invisible to the human eye, obscured by the bone. The radiologist, understandably, misses it.
If an AI is running in the background, it doesn’t suffer from visual overlap. It mathematically separates the “rib bone numbers” from the “lung tissue numbers.” It spots the 3-millimeter anomaly instantly, throws a bright red circle around it, and halts the radiologist.
“Wait,” the AI essentially says. “Look closer right here.”
The radiologist zooms in, confirms the nodule, and orders a biopsy. The cancer is caught at Stage 1 instead of Stage 4.
D. THE ADVANCED TECHNICAL LAYER: Inside the CNN
For the technology enthusiasts, how does the machine actually learn to do this without a human explicitly programming it?
The secret lies in a specific architecture called a Convolutional Neural Network (CNN).
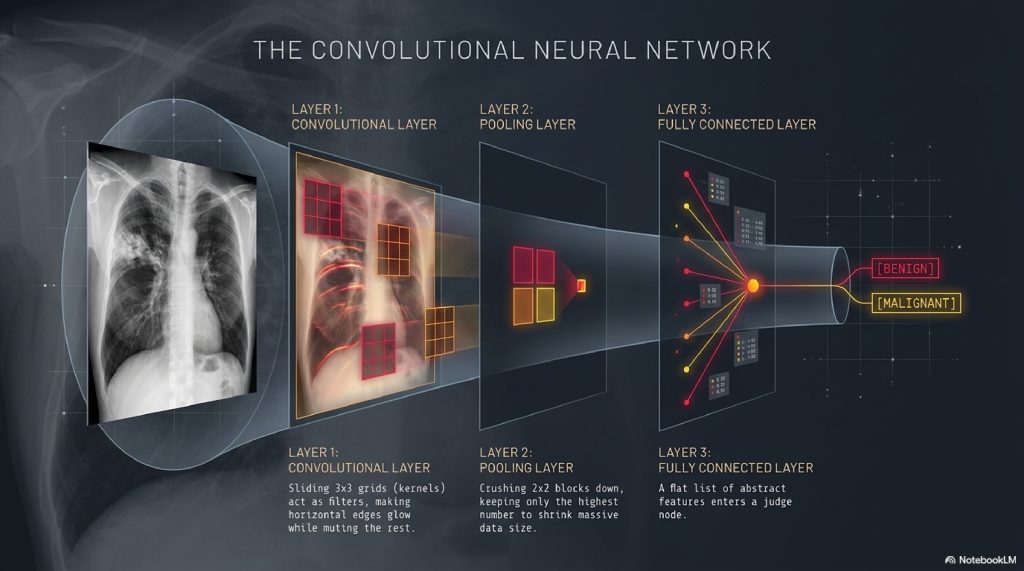
The Architecture of a CNN A CNN is inspired by the human visual cortex. It is made of multiple “hidden layers.”
- Convolutional Layer: This layer applies mathematical matrices called “kernels” to the image. A kernel might be a 3×3 grid of numbers that slides across the image. As it slides, it multiplies its numbers with the image’s pixels. This process acts like a filter, suddenly making all the horizontal edges in the image glow, while muting everything else.
- Pooling Layer: Medical images are massive. Pooling reduces the size of the data. It takes a 2×2 block of pixels, finds the highest number (the most important feature), and throws the rest away. It summarizes the image while keeping the core patterns intact.
- Fully Connected Layer: After passing through dozens of convolutional and pooling layers, the image has been broken down into a flat list of abstract features. This final layer acts as the “judge,” weighing the importance of all these features to make the final diagnosis.
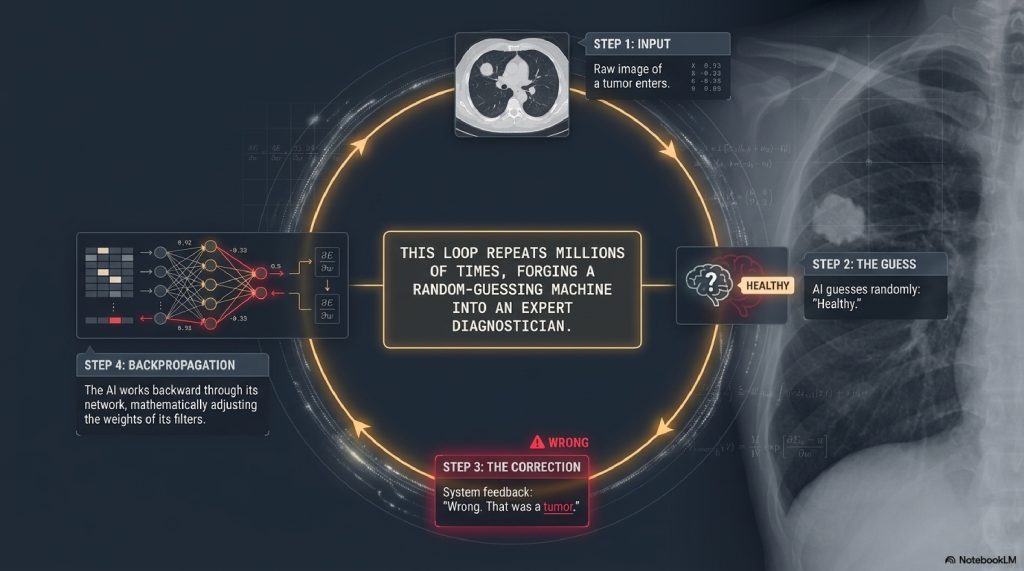
How it Learns: Backpropagation When the AI is first built, it is incredibly stupid. It guesses randomly. We feed it an image of a tumor, and it guesses “Healthy.” The system then gives it the correct answer: “Wrong. That was a tumor.” The AI then uses a mathematical algorithm called Backpropagation. It works backward through its own neural network, slightly adjusting the “weights” (importance) of its filters. It says, “Next time I see that specific curved edge, I need to weigh it more heavily toward ‘tumor’.” It repeats this process millions of times. With every single mistake, it updates its math, slowly forging itself into an expert diagnostician.
E. COMMON MYTHS ABOUT AI IN MEDICINE
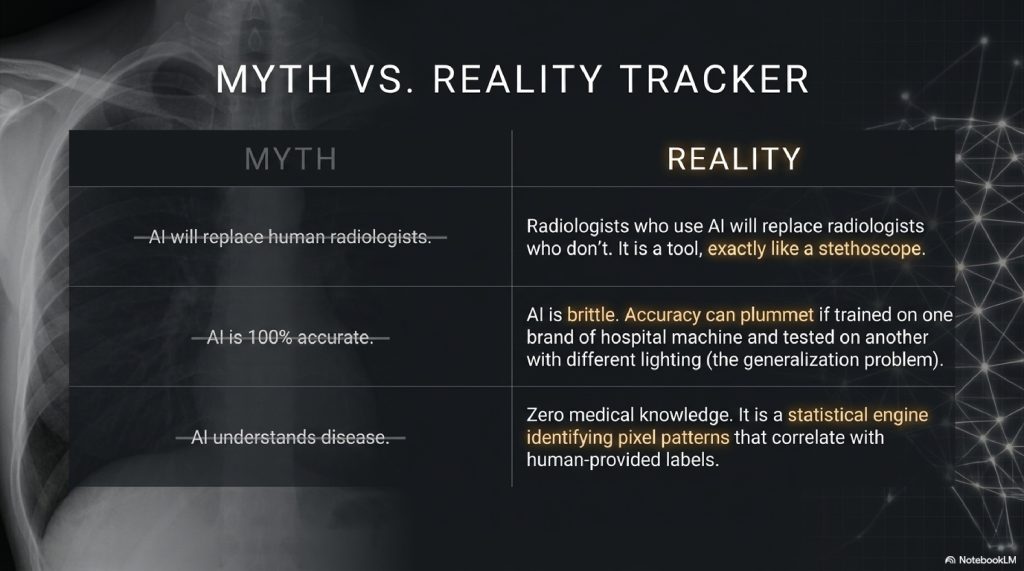
Myth 1: AI is going to replace human radiologists. Reality: There is a famous saying in the medical community today: “AI will not replace radiologists. Radiologists who use AI will replace radiologists who don’t.” An AI cannot talk to a patient, understand a complex medical history, or make a nuanced judgment call. It is a tool, exactly like a stethoscope or a scalpel.
Myth 2: AI is 100% accurate. Reality: AI is incredibly brittle. If an AI is trained exclusively on X-rays from one specific brand of hospital machine, and you feed it an X-ray from a different brand of machine with slightly different lighting, the AI’s accuracy can plummet. This is known as the “generalization problem.”
Myth 3: AI actually understands what a disease is. Reality: AI has zero medical knowledge. It doesn’t know what a lung is, or what cancer does to the human body. It is simply a statistical engine that identifies pixel patterns that correlate with labels humans have given it.
F. THE FUTURE: Predicting the Unpredictable
We are currently in the “detection” phase of AI. The machine sees what is already there. The true revolution, arriving over the next decade, is the Prediction phase.
Researchers are discovering that AI can see things in medical scans that humans have literally no biological capacity to see.
For example, scientists have fed standard retinal scans (pictures of the back of the eye) into AI models. Humans use these to look for eye disease. But the AI realized that the microscopic blood vessels in the eye contain hidden data. The AI can look at a picture of your eye and accurately predict your biological age, your gender, your blood pressure, and your risk of suffering a major heart attack within the next five years.
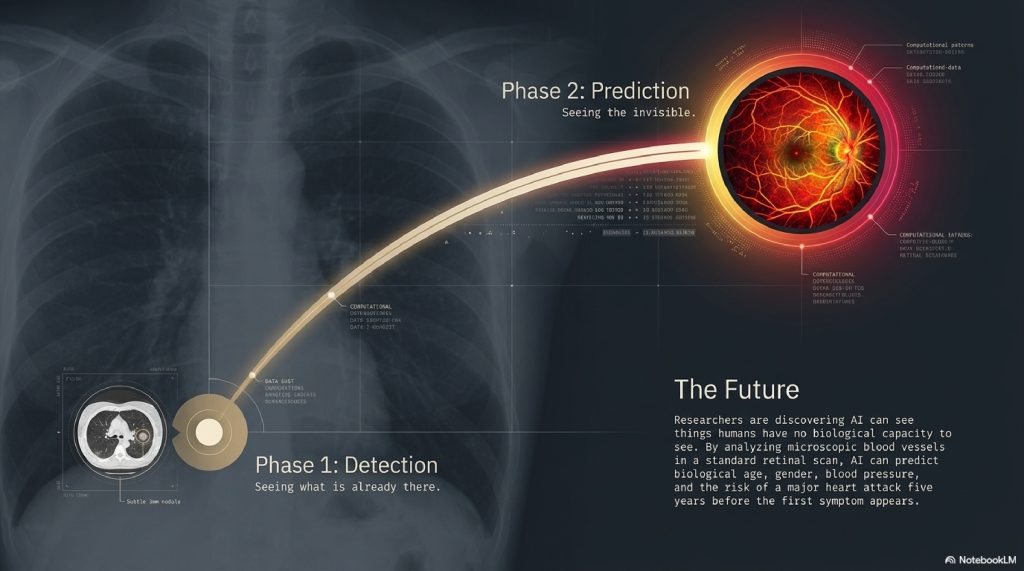
In the future, a routine scan won’t just tell you if you are sick today. It will read the microscopic, invisible topography of your tissues to map out the diseases you are likely to develop years before the first symptom ever appears.
G. INTERESTING FACTS YOU DIDN’T KNOW
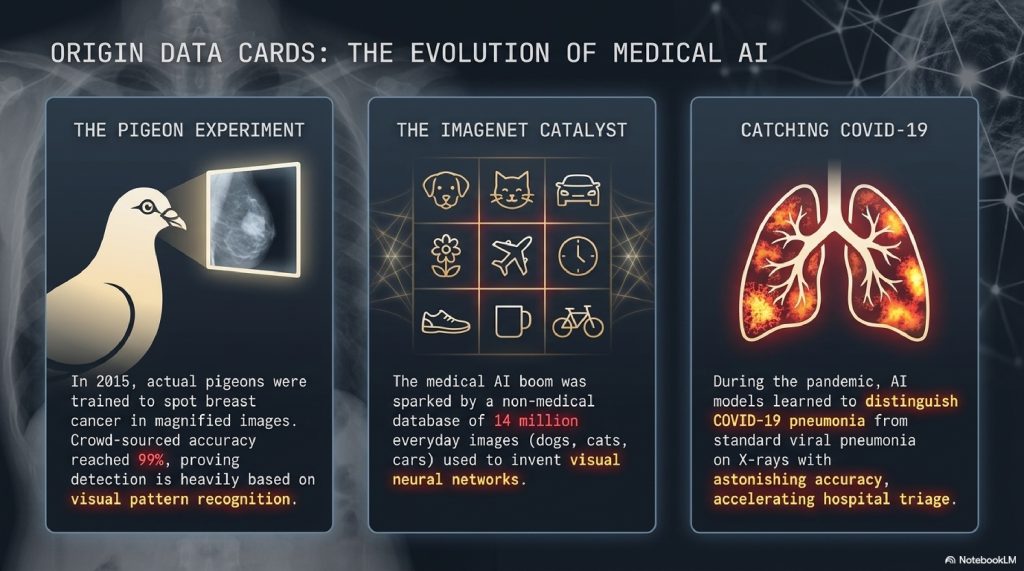
- The Pigeon Experiment: In 2015, researchers trained actual pigeons to look at magnified medical images and peck a button if they saw breast cancer. The pigeons were surprisingly accurate (up to 99% when crowd-sourced). This proved that detecting cancer is heavily based on visual pattern recognition, the exact thing AI excels at.
- The ImageNet Catalyst: The boom in medical AI was made possible by a non-medical project called ImageNet, a database of 14 million everyday images (dogs, cats, cars). Computer scientists used this database to invent the visual neural networks that were later adapted for medicine.
- Catching COVID-19: During the peak of the pandemic, AI models were developed that could look at a chest X-ray and distinguish a COVID-19 pneumonia infection from standard viral pneumonia with astonishing accuracy, speeding up triage in overwhelmed hospitals.
H. FAQ SECTION
1. Is AI currently being used in my local hospital? It is highly likely. The FDA has already approved hundreds of AI algorithms for medical imaging. Many modern radiology departments run AI software in the background to automatically triage and flag urgent cases (like brain bleeds) for immediate human review.
2. How long does it take for AI to read a scan? While a complex MRI might take a human doctor 15 to 30 minutes to meticulously review, an AI model can process the raw data and generate a heatmap of anomalies in a matter of seconds.
3. Who is liable if the AI makes a mistake? Currently, the liability remains with the human doctor. The AI is legally classified as “Clinical Decision Support” software. The human doctor has the final say and is responsible for verifying the AI’s findings.
4. Does the AI ever disagree with the doctor? Frequently. When this happens, it forces the radiologist to take a second look. Often, the AI highlights a harmless artifact (like a shadow from a rib bone), but occasionally, it catches something the doctor genuinely missed.
5. How does AI handle rare diseases? This is a major weakness. Because AI requires thousands of examples to learn a pattern, it struggles immensely to detect rare diseases where only a few dozen scans exist in the entire world. Humans are vastly superior at “few-shot learning.”
6. Can AI tell if a tumor is benign or malignant without a biopsy? AI is getting very good at predicting malignancy based on the texture and edges of a tumor (a field called radiomics), but it is not definitive. A physical tissue biopsy is still required to legally and medically confirm cancer.
7. Is patient privacy protected when training these AIs? Yes. Before medical scans are fed into neural networks for training, they undergo strict “de-identification.” All names, dates, and medical record numbers are stripped from the image metadata to comply with laws like HIPAA.
8. Can AI read ultrasounds? Yes, but it is notoriously difficult. Ultrasounds are “noisy” and highly dependent on the skill of the technician holding the wand. However, AI is now being integrated directly into ultrasound wands to guide nurses in real-time, helping them capture the perfect image of a heart or fetus.
9. Will AI make healthcare cheaper? In theory, yes. By speeding up the workflow, reducing missed diagnoses (which lead to expensive advanced-stage treatments), and allowing doctors to handle a higher volume of patients, AI has the potential to dramatically lower systemic healthcare costs.
10. What is “Explainable AI” in medicine? One problem with Deep Learning is the “Black Box” effect—the AI gives an answer, but can’t explain why it made that choice. “Explainable AI” is a new field of research focused on forcing the algorithm to show its mathematical work, so doctors can trust its reasoning, not just its output.
I. OTHER BLOG SUGGESTIONS
- How Water Treatment Plants Make Dirty Water Safe to Drink
- How Biometric Authentication Protects Your Phone & Bank
- How DNS Works: Translating Website Names into IP Addresses
- How Spacecraft Communicate Across Millions of Kilometers
J. CONCLUSION
We are standing at the threshold of a new era in human health.
For the entirety of medical history, the diagnosis of illness relied solely on the biological limits of the human eye and the immense pressure placed on the human brain. We asked our doctors to be infallible, yet we gave them an impossible volume of data to process.
Artificial Intelligence does not strip the humanity from medicine; it protects it. By taking on the grueling, microscopic burden of counting pixels and highlighting anomalies, the machine frees the physician to do what no machine ever will: look a patient in the eye, hold their hand, and devise a plan to save their life.
When we combine the cold, flawless mathematical precision of the algorithm with the empathy and contextual genius of the human doctor, we create an invincible partnership. The invisible doctor is here, hiding in the code, quietly watching the pixels, ensuring that no shadow goes unseen.
Comment